

Shoulder Anatomy – A Deep Dive
The shoulder is a complex structure with several moving joints that must work in a coordinated fashion to produce movement. From here forward I want you to think of your shoulder as a complex, not a single joint.
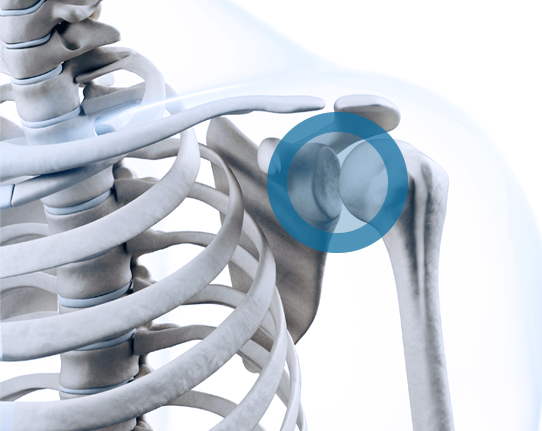
What we traditionally think of as the “shoulder joint” is referred to as the GlenoHumeral joint. This is made by the movement of two bony structures covered in articular cartilage – when I say “articular cartilage,” think of that shiny, slippery white substance on the ends of chicken bones – the glenoid and the humeral head. The glenoid is a golf tee-shaped extension of your scapula. The humeral head is a golf ball-shaped structure that is at the top of your arm bone. We will return to this “golf ball on a tee” metaphor later, so keep it in mind. However, the “glenohumeral joint” is only responsible for roughly 2/3 of the motion produced in your shoulder complex. Just like a golf ball on a tee on a windy day, it will fall off without assistance by the many soft tissue structures – tendons attached to muscles and ligaments connecting bony structures – it will fail and cause dysfunction leading to pain—much more on this below.
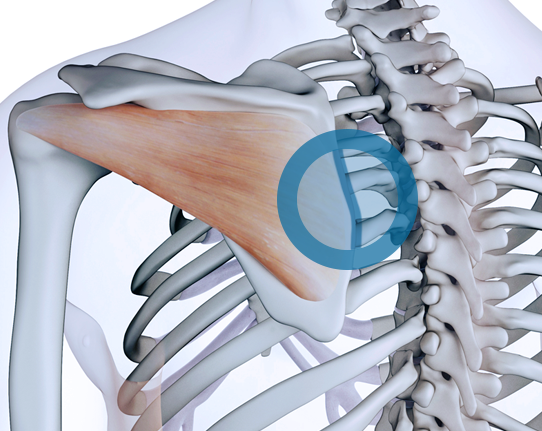
The second major joint in our shoulder complex is created by your scapula (or wing bone on the back of your shoulder complex) and your rib cage. This is referred to as the Scapulothoracic joint—”Scapulo” for the scapula, “Thoracic” for the chest. We, orthopaedists, love sensical names for structures. This is simply the joint created by the sliding of your scapula on your rib cage and is especially important at the higher ends of your range of motion, for example, reaching your arm above your shoulder. Many muscles must act in a very complex coordinated fashion to get this movement right. Think of all the coordination it takes to execute a successful drive off the tee, a play in football (American or International), hockey, or a dance troupe performing a complex sequence; without each part performing as it should, the movement fails. Failure means dysfunction and pain.
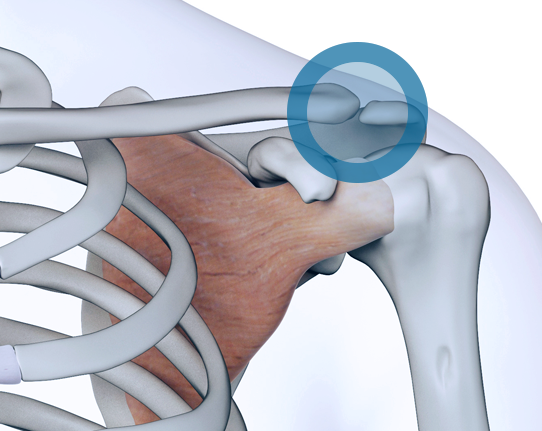
Finally, we have the acromioclavicular joint. “Acromio” stands for your acromion. Feel the outer border of the top of your shoulder. That bony protrusion is the acromion, and it is a curved structure that is a part of your scapula. The “Clavicular” stands for your clavicle or collar bone. Your clavicle is an “S” shaped bone and has a highly complex function and movement. It serves as the attachment point for the axial skeleton (think spine) and appendicular skeleton (fancy word for your extremities – arms in this case). We see many degenerative changes (arthritis is an example of a degenerative change) at this location in almost all patients. Those who perform repetitive overhead motions or heavy lifting very commonly have symptoms at this location. When people fall on their shoulders, as is common in football, they can dislocate this joint. This is commonly referred to as a “shoulder separation”. There are several grades of this injury, and most do not require surgery.
The above is the overview of the bony joints that make up the shoulder complex, simple, right? Well, if you felt it was a bit complex, you are not alone. Use the above as a reference as we move along.
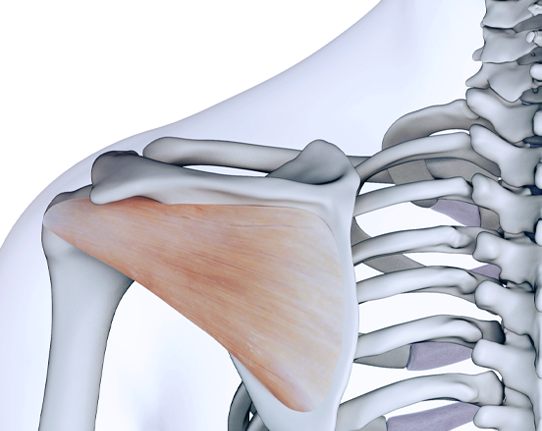
Several soft tissue structures stabilize the shoulder so the larger muscles of your shoulder, back, and chest can move your arm in space. Contrary to popular belief, the rotator cuff muscles – of which there are four – do not produce significant movements of your shoulder beyond rotation. Rather, they keep that golf ball on the tee so the larger deltoid, pectoralis major, and latissimus dorsi can move your arm in space. There are several smaller players, but we won’t complicate an already confusing issue.
The Shoulder
What is the Rotator Cuff?
A common question I get is, “What is the rotator cuff?” A rotator cuff is a group of four muscles whose predominant job is keeping the golf ball on the tee through a balanced compressive force.
More specifically, they act in a balanced fashion to give your shoulder a stable pivot point so those larger muscles can move your arm over your head from the front and side, reach behind you, or grab something overhead. The rotator cuff muscles also play a prominent role in scratching that itch in the middle of your back, setting up a forehand in tennis, washing your hair, or many other activities. The key here is when one or more of these muscles, more commonly their respective tendons, are injured, and the balance is lost. This imbalance produces abnormal movement leading to dysfunction, and pain.
Beyond the Rotator Cuff
Beyond the rotator cuff muscles, we have structures that exist inside your glenohumeral joint. We will limit our discussion to your labrum, capsule, glenohumeral ligaments, biceps tendon, and cartilage itself.
The Shoulder
The Labrum
Let’s start with the labrum. The labrum is made of a different type of cartilage that covers the ends of bones. This is both a stabilizing structure and, more importantly, an attachment point for other structures such as the capsule, ligaments, and the biceps tendon (of which there are two – the long head is what we talk about here).
The labrum is firmly attached to the bony glenoid – our golf tee – it provides a bumper type function, and itself serves only a small amount of stabilization. It becomes more important as an attachment site for more critical stabilizing structures, specifically the capsule and its ligaments. More on these structures later. The labrum can become injured and produce a variety of symptoms. Very commonly, tears occur near or at the site where the biceps tendon inserts. This is referred to as a SLAP tear. A SLAP tear is an acronym standing for Superior Labrum Anterior to Posterior, just a description of the tear really, and has many, many different subtypes. The most important consideration is that it can cause pain, especially in overhead athletes – tennis players, swimmers, baseball and softball players, etc. The treatment for these injuries has changed significantly in the last fifteen years. Frankly, most do not need repair, but rather a biceps tenodesis – where we disconnect the biceps tendon and “plug it in” to the groove in your upper arm bone where it runs- is the modern treatment. Who gets repairs? High-level overhead athletes under the age of 35 years. High level means professional or collegiate in my world. Every case is different, but the literature does not support the repair of most SLAP tears in other individuals above the age of 35.
Labral tears are also common in patients who suffer from shoulder instability or dislocation. It is here where we need to discuss the capsule and its ligaments. The “ligaments” in the shoulder are actually thickenings of the shoulder capsule. Think of this as a continuous sheet of stabilizing tissue that is thicker in specific locations. This allows different parts of the capsuloligamentous complex to be active in different shoulder positions. When patients dislocate their shoulder, it is very common to tear certain areas of this complex depending on how they dislocate their shoulder. If the instability continues despite physical therapy, activity modifications, and/or technique improvement, we discuss repairing these structures. In certain cases, patients also have an injury to the bones in the shoulder, and different strategies are employed – the complexity of which is beyond what we will discuss here.
Our discussion aims to lay out a road map to the many structures in your shoulder, which can cause dysfunction and pain when they are injured. It can be as confusing as the rules of golf, so don’t let it frustrate you. I am here to both educate and execute the treatment strategy that will best accomplish your goals.